
In the hospital, I see the same story play out every night. A patient can’t sleep, and they ask for “the good stuff.”
But in sleep medicine, “good” is a complicated word. Does “good” mean it knocks you out the fastest? Or does “good” mean you can stop taking it without having a seizure?
As an internal medicine resident, I use a mental “Safety Hierarchy” when deciding what to prescribe. We always start with the safest, least addictive options and only move up the ladder when absolutely necessary.
Here is the unvarnished truth about the three most common classes of sleep aids: Trazodone, Z-Drugs, and Benzos.
Level 1: Trazodone (The “Clinical” Favorite)
If you tell your primary care doctor you have insomnia, you will likely leave with a prescription for Trazodone.
What it is: Trazodone is actually an antidepressant, approved in the 1980s. At high doses (300mg+), it treats depression. But at low doses (50mg-100mg), it acts as a sedative by blocking Histamine (H1) and Alpha-1 Adrenergic receptors.
The “Resident Insight”: Here is the conflict: The American Academy of Sleep Medicine (AASM) actually suggests against using Trazodone for insomnia because the data on its efficacy is weak.
- Why we prescribe it anyway: It is non-addictive. You do not build up a tolerance to it, and it is not a controlled substance. For a doctor, it is the “safest” pill to write for long-term use.
The Risks:
- The “Hangover”: It has a long half-life, meaning it often leaves people feeling groggy the next morning.
- Orthostatic Hypotension: It can drop your blood pressure when you stand up (a fall risk for the elderly).
- Priapism: A rare but serious side effect where men experience a painful, prolonged erection requiring emergency treatment.
Level 2: The “Z-Drugs” (Ambien, Lunesta, Sonata)
If Trazodone doesn’t work, we move to the Sedative-Hypnotics, affectionately known as “Z-Drugs” (because they all have Zs: Zolpidem, Eszopiclone, Zaleplon).
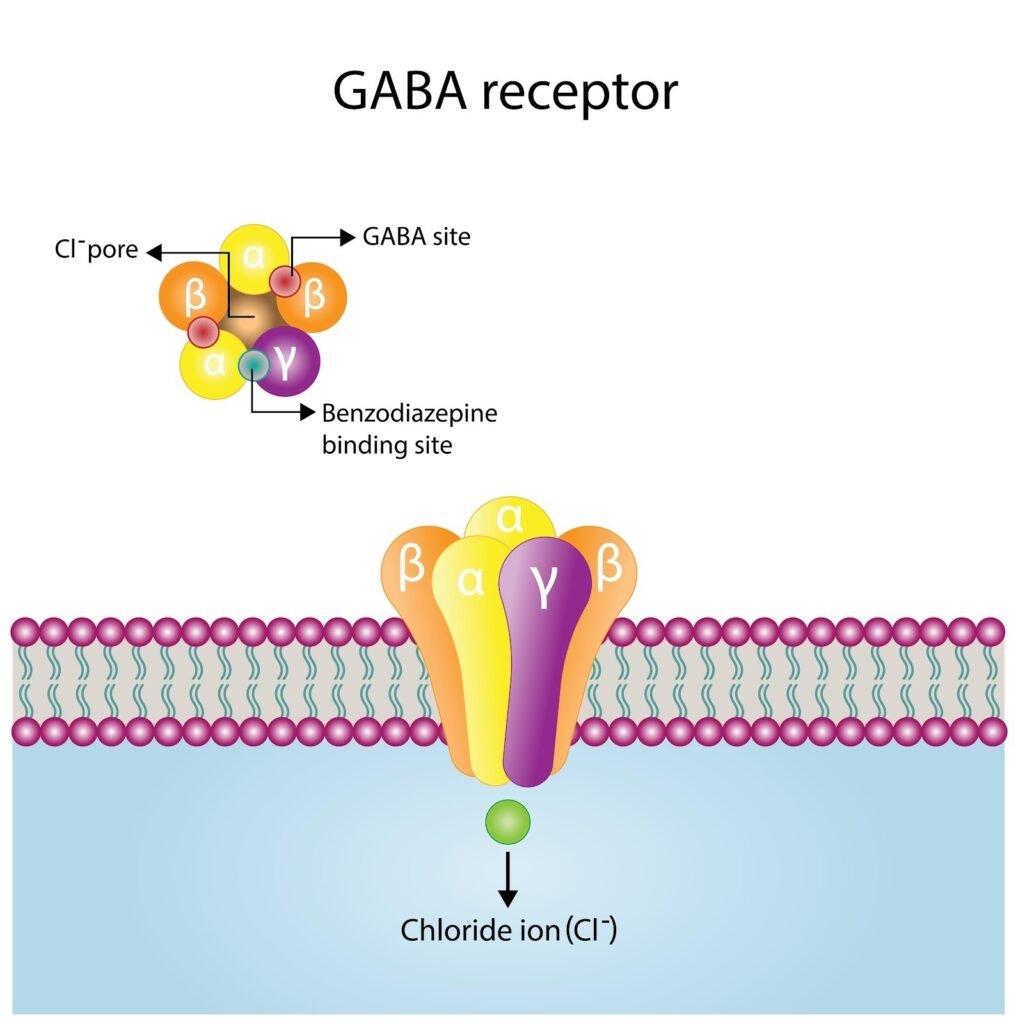
What they are: These are “specialists.” Unlike Trazodone (which is a dirty drug that hits many receptors), Z-Drugs are designed to do one thing: hit the GABA-A receptor to shut your brain off.
The Pros:
- They Work: They are FDA-approved for insomnia because they are highly effective at initiating sleep.
- Cleaner Sleep: They tend to preserve your “sleep architecture” (your deep sleep and REM stages) better than benzodiazepines.
The Risks:
- Complex Sleep Behaviors: This is the big one. Z-Drugs carry an FDA Black Box Warning for causing sleep-walking, sleep-eating, and even sleep-driving.
- Dependence: While safer than Valium, you can become dependent on them. Rebound insomnia (worse sleep when you stop) is common.
Level 3: Benzodiazepines (The “Nuclear Option”)
This category includes drugs like Xanax (Alprazolam), Ativan (Lorazepam), Valium (Diazepam), and Temazepam.
What they are: Benzos are heavy-duty anxiolytics (anti-anxiety meds). They slam the GABA receptor wide open.
In 2025, we rarely write new prescriptions for benzodiazepines for chronic insomnia. They are generally reserved for:
- Acute Panic/Grief: If someone just lost a spouse and hasn’t slept in 3 days.
- Short-Term Use: Less than 2 weeks.
The Risks (Why they are at the bottom of the hierarchy):
- Tolerance: They stop working fast. You might need 1mg today, but in a month, you’ll need 2mg to get the same effect.
- Altered Architecture: Benzos might keep you unconscious, but they steal your Deep Sleep (Stage N3). You wake up unconscious, but not restored.
- The Withdrawal: Benzodiazepine withdrawal is one of the few withdrawals (along with alcohol) that can actually kill you via seizures.
The PillowTalkMD Verdict
Pills are tools, not cures.
- If you need something safe for long-term use and don’t mind mild grogginess, Trazodone is often the first stop.
- If you have severe, short-term insomnia, a Z-Drug is the sharpest tool, but requires respect.
- Benzodiazepines should be treated like fire: useful in an emergency, but dangerous to play with.
But remember: The only “cure” for insomnia that sits at the very top of the hierarchy isn’t a pill at all. It’s CBT-I.
Disclaimer: The content on this blog is for informational and educational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider.


